

The Metabolic Crisis Is Not a News Story
It's Your Neighbor, Your Friend, Possibly You.

By Steven Muskal, Ph.D. | May 6, 2026 | stevenmuskal.com

Think about the people you know well. Your family, your close friends, the colleagues you’ve worked alongside for years. How many of them are managing diabetes or prediabetes right now? How many are carrying it without knowing? How many are metabolically struggling in ways that haven’t yet been named or diagnosed?
I grew up in a world where diabetes was something you heard about in passing. There might have been one person in your extended circle. Type 2 barely entered the conversation. It was the kind of condition that felt distant, clinical, abstract. Now it is everywhere. Not on the news as some faraway epidemic. In the room with you. At the dinner table. In the family group chat.
That shift did not happen gradually enough that we noticed it arriving. It happened across a generation, in plain sight, while we were busy with other things. And what I find remarkable, and genuinely troubling, is that the numbers continue to accelerate.
A Number That Should Startle You
More than 38 million Americans currently have diabetes, representing about 11.6 percent of the entire US population. Another 98 million Americans have prediabetes, the majority of whom are unaware of it. Put those numbers together and you are looking at roughly a third of the country at some stage of glucose dysregulation.
Globally, the picture is equally striking. According to the World Health Organization and data published in The Lancet in late 2024, the number of adults living with diabetes worldwide has surpassed 800 million, more than quadrupling since 1990. Not doubling. Quadrupling. In roughly one human generation.
But the statistic that genuinely stopped me when I first encountered it comes from a 2018 study by researchers at the University of North Carolina: only about 12 percent of American adults meet criteria for optimal metabolic health, defined as healthy levels of blood sugar, triglycerides, HDL cholesterol, blood pressure, and waist circumference without the use of medications. A 2022 study from Tufts University put that figure even lower, at approximately 7 percent.
Seven to twelve percent. That means somewhere between 88 and 93 percent of American adults are operating with at least one metabolic risk factor.
To put that in historical context: Type 2 diabetes was considered a rare condition in the mid-twentieth century. Physicians who trained in the 1950s and 1960s might have encountered a handful of cases across their entire careers. It was classified as a disease of older age, of significant excess weight, of unusual circumstances. The phrase “Type 2 diabetes” barely existed in public vocabulary. Now it is discussed in middle schools. Pediatric endocrinologists have waiting lists. The disease that was once rare enough to be remarkable has become so common that we have largely stopped remarking on it.
What changed?
The Drivers We Talk About, and the Ones We Don’t
The conventional explanation focuses on diet and physical activity. Ultra-processed foods now constitute the majority of calories consumed in the United States. Studies tracking the rise of industrial food processing point to refined carbohydrates, seed oils, and the engineered palatability of products specifically designed to override our natural satiety signals. Portion sizes expanded. Caloric density increased. Fiber largely disappeared. The metabolic consequences followed.
Sedentary behavior amplified the effect. Office work, car commuting, streaming entertainment, and smartphones conspired to reduce the amount of time most adults spend in genuine physical activity. Not dramatically for any single generation, but cumulatively across decades.
Sleep is another factor that gets less attention than it deserves. The research connecting sleep deprivation to insulin resistance, metabolic dysregulation, and weight gain is substantial and growing. I wrote about this at length in an earlier piece on measuring and managing sleep. When you do not sleep well, your body’s ability to process glucose deteriorates. Chronically. A population that sleeps significantly less than it did fifty years ago is also a population primed for metabolic dysfunction.
Chronic stress belongs in this conversation too, though it tends to be treated as a soft variable. Cortisol dysregulation affects blood sugar. The constant low-grade alertness that comes from always-on digital life, economic precarity, and the particular anxiety of watching the world move faster than we can process is not neurologically benign. Neither is the dopamine disruption from screen-based reward loops, which increasingly correlates with disrupted eating patterns, sleep fragmentation, and reduced motivation for physical movement.
There is also a less-discussed category: environmental contributors. Some researchers have begun examining the correlation between industrial chemical production and diabetes incidence, including endocrine-disrupting compounds in food packaging, pesticide residues, and pollutants that may interfere with metabolic signaling. The evidence here is still accumulating, and causation is difficult to establish. But the correlation curves are hard to ignore.
None of these factors operates in isolation. They interact with each other, compound across time, and land differently depending on genetics, access, and circumstance. The honest answer to what changed is: almost everything, almost simultaneously, over about fifty years.
The Trauma Thread
I want to raise a question here that I do not think gets nearly enough attention, and that I’m not in a position to answer definitively. It is more of an observation that has been sitting with me since a conversation I had on my podcast last year.
Christy Shearer joined me to talk about her experience living with Type 1 diabetes. You can listen to that conversation here. Among the many things she shared, one observation in particular stayed with me. She noted, anecdotally, that many of the people she knows with Type 1 experienced significant trauma in the period preceding their diagnosis. Not minor stress. Significant, life-disrupting events. Big-T trauma, as some clinicians describe it.
Type 1 diabetes is an autoimmune condition. The immune system turns against the insulin-producing beta cells of the pancreas. We know that autoimmune disorders can be triggered or accelerated by stress and trauma. The HPA axis, which governs the body’s stress response, is deeply interwoven with immune regulation. Prolonged activation of that system, as occurs in response to unresolved trauma, produces measurable changes in inflammatory signaling and immune function.
Is there a connection between rising rates of psychological trauma in our society and rising rates of autoimmune-mediated Type 1 diabetes? I do not know. The research is genuinely complex, and I want to be careful not to overstate the case. But the incidence of Type 1 in youth has been increasing measurably over recent decades, even as our understanding of why remains incomplete.
What I feel more confident saying is this: chronic stress, whether sourced in trauma, financial insecurity, social isolation, or the ambient pressure of modern life, is a metabolic disruptor in ways that cut across both Type 1 and Type 2. The stress-insulin-glucose feedback loop is real. It is understudied in public health framing. And it is probably not unrelated to the trends we are seeing.
The Network Effect of Metabolic Health
One of the most striking pieces of research I have encountered on this topic comes from a landmark 2007 study in the New England Journal of Medicine by Nicholas Christakis and James Fowler. They analyzed a social network of over 12,000 people tracked across 32 years and found that obesity appears to spread through social ties in ways that mirror how contagious diseases propagate. If someone in your immediate social network became obese, your own risk of becoming obese increased by roughly 57 percent. The effect was strongest among mutual friends, weakened with geographic distance, and was not explained by shared environmental factors alone.
The mechanism they proposed is social norms. When the people around you change their behaviors, their relationship to food, their activity level, even their body size, it shifts what feels normal. And once a behavior feels normal, it becomes easier to adopt without conscious decision-making.
The reverse, I think, is also true. When someone in your network starts to pay attention, starts measuring, starts making visible changes, the ripple moves in that direction too. I have seen this in small ways in my own life. When I began tracking my sleep seriously and started talking about what I was learning, several people in my circle started paying more attention to theirs. The conversation changes what seems worth doing.
This is actually one of the core motivations behind the tools I have been building. Not just personal optimization, but the possibility that visible, shared attention to health can propagate through a network in a more useful direction than the metabolic drift we’ve watched unfold over the past few decades.
CGMs Are No Longer Just for Diabetics
A Continuous Glucose Monitor, or CGM, is a small sensor worn on the upper arm or abdomen that reads blood glucose levels in real time, typically every five minutes, and transmits those readings to a phone. For people managing insulin-dependent diabetes, they are genuinely life-altering technology. But something interesting has been happening over the past several years: CGMs have become increasingly available to people with no diabetes diagnosis at all, as lifestyle and performance tools.
I tried two of them. My experience was instructive, and my preference was clear.
I used NutriSense, which runs on the Abbott FreeStyle Libre sensor, a 14-day wear. I also tried Levels, which uses the Dexcom G7, a 10-day sensor. Both gave me genuinely useful data. But the experiences were meaningfully different.
NutriSense won, for me, on the app. It is cleaner, more lifestyle-oriented, and importantly, it does not require your phone to be physically present to collect readings. The Libre sensor stores data locally and syncs when you’re ready. That matters if you are not looking for your phone to be a permanent extension of your body during the experiment.
Levels felt more clinically calibrated, designed closer to the diabetic management model. It was more alert-heavy, flagging glucose levels that, from a lifestyle perspective, were entirely unremarkable. If your glucose dips to 70 while fasting and you feel fine, an alarm at 70 (early a.m.) is not useful information. For someone managing active insulin sensitivity and metabolic disease, that threshold is medically appropriate. For lifestyle tracking, it created noise I did not need.
The practical accessibility of this technology has also shifted significantly. You can now purchase a CGM directly on Amazon without a prescription for lifestyle use. The barrier to trying one, if you are curious about your metabolic responses to food, exercise, stress, or sleep disruption, is lower than it has ever been. I would recommend it to almost anyone who is serious about understanding their metabolic baseline.
You Cannot Optimize What You Do Not Observe
This is the core principle behind everything I have been building in my personal AI system, which I have written about elsewhere under the name AI/Steve. The premise is simple: if you want to change something about your health, you need to see it first. Measurement precedes management. Observation enables intention.
I applied this logic to sleep, building a framework to track, analyze, and improve sleep quality over time. I wrote about that process in an earlier piece on measuring to manage sleep. I applied it to food, exploring how meal data could close the loop between behavior and biology, which I covered in depth in Food Is Medicine. But First It Has to Become Data.
Glucose is the natural next signal in that chain. It is one of the most responsive and informative biomarkers available for real-time feedback. It tells you things almost nothing else does: how your body is handling what you just ate, how well you recovered last night, how a stressful meeting affected your biology, whether that afternoon slump has a metabolic component. It connects the inputs, food, sleep, movement, stress, to the outputs, how you feel and how your body is functioning.
The challenge, for people who are not managing a diagnosed condition, has been the tools. CGMs give you the data stream. But without a framework to log meals alongside glucose readings, analyze patterns over time, and contextualize what you are seeing, the data is interesting but not yet actionable. That is the gap the app I have been working on is designed to close.
Introducing Food Health TxD
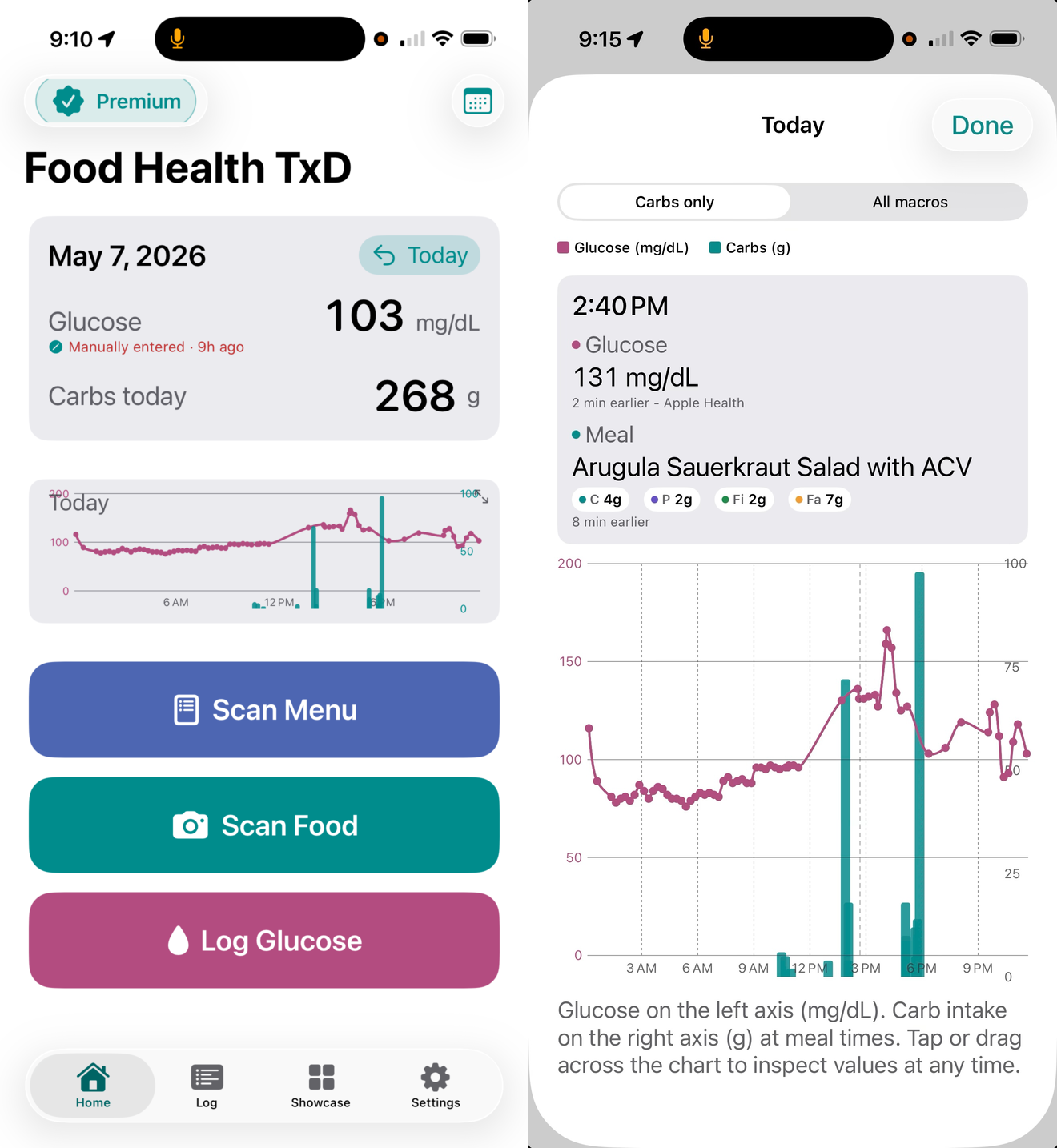
Food Health TxD is the next evolution of Food Health AI, the meal logging and nutritional analysis application I described in the Food Is Medicine article. Where the original application focused on making food logging fast and painless using photo-based AI analysis, Food Health TxD is built specifically for people who are tracking glucose alongside food intake.
The core use case is exactly what you would expect: you photograph a meal, the AI analyzes it for carbohydrates, macronutrients, and glycemic context, and the app maintains a running record of what you ate alongside your glucose readings. Over time, that creates a personal dataset that is genuinely yours. Not averages from a population study. Not recommendations from a generic guideline. Your food, your glucose, your patterns.
The application is built for a range of users. If you are managing Type 1 or Type 2 diabetes and trying to understand how specific meals affect your glucose, it gives you that picture with real data. If you have prediabetes and want to see exactly how different dietary choices affect your metabolic trajectory, that visibility is there. And if you are metabolically healthy and simply want to stay that way, or to use a CGM period as a learning experience, the app gives you the context to make sense of what you are observing.
One integration worth explaining specifically is Apple Health. Apple has taken a deliberately conservative approach to blood glucose within their Health platform. Real-time CGM streaming is not supported as a direct API integration, which is, frankly, the right call given the liability considerations around medical device data. Food Health TxD works within those constraints. Apple Health serves as the central aggregation layer for your activity data, sleep data, and manually entered glucose readings. The app does not attempt to circumvent Apple’s appropriate caution. It works alongside it.
I want to be direct about what the app is and is not. Food Health TxD is a guidance and educational tracking tool. It is not a medical device. It is not a diagnostic instrument. It does not replace clinical care, nutritional counseling, or your physician’s guidance. It is a way to see your own data more clearly and to build a personal record that can inform better questions and better conversations. That framing matters to me. I am not trying to play doctor. I am trying to give people tools to understand themselves.
If You Want to Try It
Food Health TxD is not yet in public release, and I want to be honest about where it stands. The application is in the App Store at this link, and I am actively looking for beta testers. Specifically, people who are curious about metabolic health, managing or monitoring diabetes, using or considering a CGM, or simply interested in the intersection of personal data and food. If that is you, reach out directly. You can find me through stevenmuskal.com. I would genuinely like to hear what you are trying to understand about your own metabolic health, and I am interested in building the tool around real use cases, not hypothetical ones.
The Bet
Let me come back to where we started. Almost everyone reading this knows someone managing a metabolic condition. Some of you are managing one yourselves. The numbers we are looking at are not projections about a future possibility. They are descriptions of a present reality that most of us are already living inside.
What I believe, and what the research on social network effects supports, is that the metabolic crisis is not inevitable at the individual level. It is largely a product of environment and behavior, and both of those are, to varying degrees, responsive to awareness and choice. Not every case, not without difficulty, and not without acknowledging the real structural factors, food access, economic stress, healthcare gaps, that make individual optimization harder for some than for others.
But awareness matters. Measurement creates awareness. And when one person in a network starts paying attention, starts seeing their data, starts having different conversations about food and sleep and glucose, the people around them tend to notice. That is not a guarantee. It is a pattern. And it is a pattern worth betting on.
The metabolic crisis arrived quietly, across decades, one small behavioral shift at a time. The path back, if there is one at the population level, probably runs through a similar kind of quiet, incremental change. One person. One measurement. One conversation. Repeated at scale, across networks, over time.
That is what I am building toward. I hope it is useful to you.
For a mix - I thought this one from a previous session might be appropriate. Grant leading (vocals/guitar), Randi (Vocals), Andrew (Guitar), Alan (Bass). Johhny (Congas)
About the Author
Steven Muskal, Ph.D., is CEO of Eidogen-Sertanty, a pioneer in AI-driven drug discovery since the early 1990s, and the creator of the Food Health and Food Health TxD applications. He writes about science, health, entrepreneurship, and the art of paying attention at stevenmuskal.com and on Substack.
Related Reading
Food Is Medicine. But First It Has to Become Data. (Substack) | Medium version
Optimizing Sleep: Measure to Manage
Glucose, Grit and Breaking Glass Ceilings (with Christy Shearer)
This article is for informational and educational purposes only. Nothing here constitutes medical advice. Consult your physician before making changes to your diet, health monitoring, or treatment plan.
Excellent ideas and writing!